Welcome to Trainer's Choice's patient resource about Acromioclavicular Joint Separation.
A shoulder separation is a fairly common injury, especially in certain sports. Most shoulder separations are actually injuries to the acromioclavicular (AC) joint. The AC joint is the connection between the scapula (shoulder blade) and the clavicle (collarbone). Shoulder dislocations and AC joint separations are often mistaken for each other. But they are very different injuries.
This article will help you understand:
what the AC joint is
what happens when the AC joint is separated
how an AC joint separation is treated.
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Shoulder Pain|limit:15|heading:Hear from some of our patients who we treated for *Shoulder Pain*#
Anatomy
What is the AC joint, and how does it work?
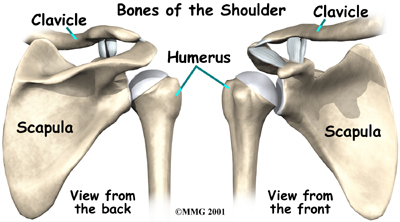
The shoulder is made up of three bones: the scapula (shoulder blade), the humerus (upper arm bone), and the clavicle (collarbone).
Shoulder Bones
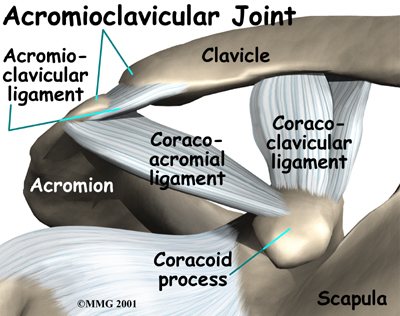
The part of the scapula that makes up the top of the shoulder is called the acromion. The AC joint is where the acromion and the clavicle meet. Ligaments hold these two bones together.
Acromion
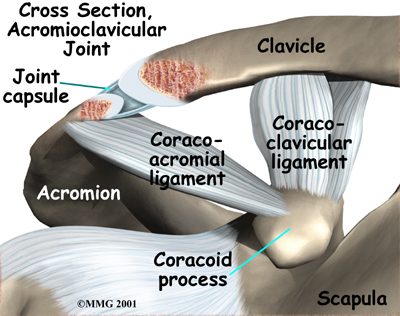
Ligaments are soft tissue structures that connect bone to bone. The AC ligaments surround and support the AC joint. Together, they form the joint capsule. The joint capsule is a watertight sac that encloses the joint and the fluids that bathe the joint. Two other ligaments, the coracoclavicular ligaments, hold the clavicle down by attaching it to a bony knob on the scapula called the coracoid process.
Joint Capsule
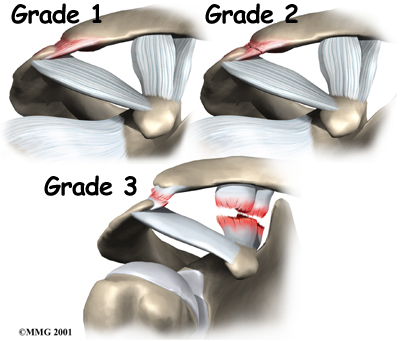
AC joint separations are graded from mild to severe, depending on which ligaments are sprained or torn. The mildest type of injury is a simple sprain of the AC ligaments. Doctors call this a grade one injury. A grade two AC separation involves a tear of the AC ligaments and a sprain of the coracoclavicular ligaments. A complete tear of the AC ligaments and the coracoclavicular ligaments is a grade three AC separation. This injury results in the obvious bump on the shoulder.
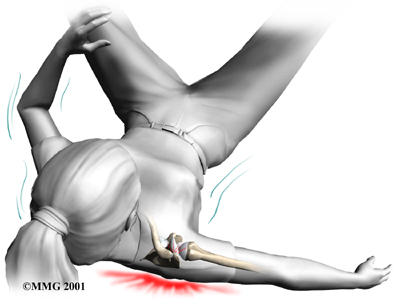
The most common cause of an AC joint separation is falling on the shoulder. As the shoulder strikes the ground, the force from the fall pushes the scapula down. The collarbone, because it is attached to the rib cage, cannot move enough to follow the motion of the scapula. Something has to give. The result is that the ligaments around the AC joint begin to tear, separating (dislocating) the joint.
Symptoms range from mild tenderness felt over the joint after a ligament sprain to the intense pain of a complete separation. Grade two and three separations can cause a considerable amount of swelling. Bruising may make the skin bluish several days after the injury.
In grade three separations, you may feel a popping sensation due to shifting of the loose joint. Grade three separations usually cause a noticeable bump on the shoulder.
How will my health care provider diagnose my problem?
When you visit Trainer's Choice, our physiotherapist will need to get information about your injury and a detailed medical history. You will need to answer questions about past injuries to your shoulder. We may ask you to rate your pain on a scale of one to 10.
Diagnosis is usually made by the physical examination. Our physiotherapist may move and feel your sore joint. This may hurt, but it is very important that we understand exactly where your joint hurts and what movements cause you pain.
Some patients may be referred to a doctor for further diagnosis. Once your diagnostic examination is complete, the physiotherapists at Trainer's Choice have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Trainer's Choice provides services for physiotherapists in North America.
If you don't need surgery, your physiotherapist at Trainer's Choice will have you begin range-of-motion exercises as your pain eases, followed by a program of strengthening. At first, we’ll have you do exercises with your arm kept below shoulder level. Our program will then advance to include strength exercises for the rotator cuff and shoulder blade muscles. In most cases, the pain goes away almost completely within three weeks. Although the time required for rehabilitation varies, full recovery can typically take up to six weeks for grade two separations and up to 12 weeks for grade three separations. Since there is little danger of making the condition worse, you can usually do whatever activities you can tolerate.
Post-surgical Rehabilitation
You may have to wear a sling to support and protect the shoulder for a few days. When you begin your physiotherapy rehabilitation program, the first few physiotherapy treatments will focus on controlling the pain and swelling from surgery. Ice and electrical stimulation treatments may help. Our physiotherapist may also use massage and other types of hands-on treatments to ease muscle spasm and pain.
We will usually wait four weeks before starting range-of-motion exercises. Our physiotherapist will probably have you begin with passive exercises. In passive exercises, we will move your shoulder joint while your muscles stay relaxed. Our physiotherapist will gently move your joint and gradually stretches your arm. You may be taught how to do passive exercises at home.
Active therapy usually starts six to eight weeks after surgery, giving the ligaments time to heal. Active range-of-motion exercises help you regain shoulder movement using your own muscle power. Our physiotherapist might have you begin with light isometric strengthening exercises. These exercises work the muscles without straining the healing joint.
After about three months, you can usually start more active strengthening. These exercises will focus on improving strength and control of the rotator cuff muscles and the muscles around the shoulder blade. Our physiotherapist will help you retrain these muscles to keep the ball of the humerus centered in the socket. This helps your shoulder move smoothly during all your activities.
Recovery from shoulder surgery can take some time. You will need to be patient and stick to your therapy program. Some of the exercises that we'll recommend are designed get your shoulder working in ways that are similar to your work tasks and sport activities. Our therapist will help you find ways to do your tasks that don't put too much stress on your shoulder. Before your physiotherapy sessions end, our physiotherapist will teach you a number of ways to avoid future problems.
Trainer's Choice provides services for physiotherapy in North America.
Your doctor may order X-rays. X-rays can show an AC joint disruption, and they may be necessary to rule out a fracture of the clavicle. In some cases, X-rays are taken while holding a weight in each hand to stress the joint and show how unstable it is.
Treatment for a grade one or grade two separation usually consists of pain medications and a short period of rest using a shoulder sling. The treatment of grade three AC separations is somewhat controversial. Many studies show no difference whether a person is treated with surgery or conservative treatment. Even with surgery, a bump may still be present where the separation occurred. And a significant portion of people who undergo surgery will need another operation later.
Several studies have looked at what happens to the AC joint after this injury. It appears that many people, whether they had the joint repaired surgically or not, will need an operation at some time in the future. The injured joint degenerates faster than normal. Over time it becomes arthritic and painful. This process may take years to develop, but sometimes it happens within one or two years.
Some surgeons prefer to repair severe grade three AC separations, especially in high-level throwing athletes.
View animation of surgery:
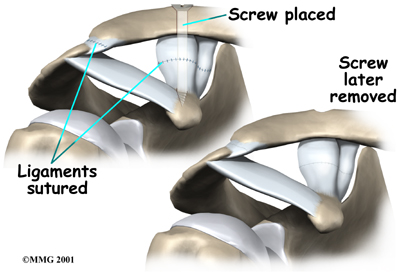
The surgery is usually done through a four-inch incision over the AC joint. The surgeon starts by putting the joint into its correct position. A screw or some other type of fixation may be used to hold the clavicle in place while the ligaments heal.
To fix the joint using a screw, the surgeon inserts the screw through the top of the clavicle and into the coracoid process.
Some surgeons use surgical tape to connect the clavicle and coracoid. A small drill hole is made in the clavicle and corocoid. The surgical tape is looped through each hole and pulled snugly.
In some cases, sutures are also used to repair and reinforce the torn coracoclavicular ligaments.
When a screw is used, it is usually removed six to eight weeks after the surgery. If it is not removed, the screw will probably break.