Introduction
Physiotherapy in North America for Knee
Welcome to Trainer's Choice's patient resource about Osteoarthritis of the Knee.
Osteoarthritis (OA) is a common problem for many people after middle age. OA is sometimes referred to as degenerative, or wear and tear, arthritis. OA commonly affects the knee joint. In fact, knee OA is the most common cause of disability in North America. In the past, people were led to believe that nothing could be done for their problem. Now there are many ways health professionals like physiotherapists can treat knee OA so patients have less pain, better movement, and enhanced quality of life.
This guide will help you understand:
- how OA develops
- how OA of the knee causes problems
- how doctors treat the condition
#testimonialslist|kind:all|display:slider|orderby:type|filter_utags_names:Knee Pain|limit:15|heading:Hear from some of our patients who we treated for *Knee Pain*#
Anatomy
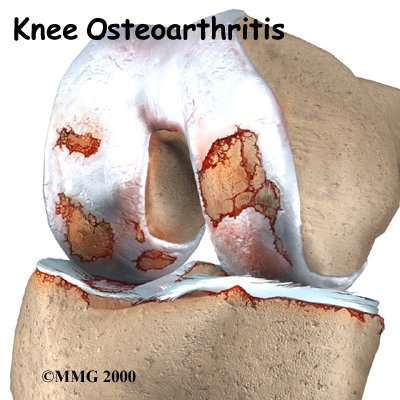
Which parts of the knee are affected?
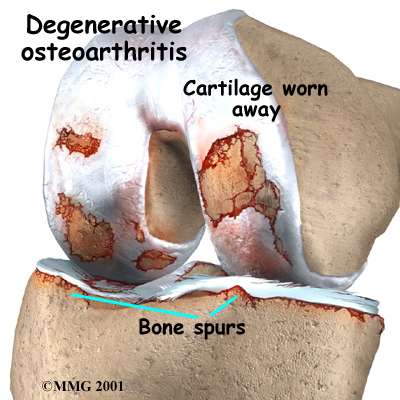
The main problem in OA is degeneration of the articular cartilage. Articular cartilage is the smooth lining that covers the ends of the leg bones where they meet to form the knee joint. The cartilage gives the joint freedom of movement by decreasing friction. The the articular cartilage is called subchondral bone.
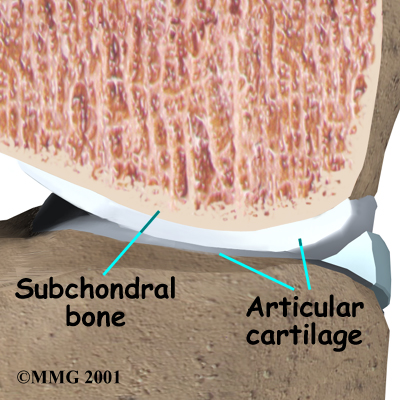
When the articular cartilage degenerates, or wears away, the bone underneath is uncovered and rubs against bone. Small outgrowths called may form in the joint.
Related Document: Trainer's Choice's Guide to Knee Anatomy
Knee Anatomy Introduction
Causes
How does knee OA develop?
OA of the knee can be caused by a knee injury earlier in life. It can also come from years of repeated strain on the knee. Fractures of the joint surfaces, ligament tears, and meniscal injuries can all cause abnormal movement and alignment, leading to wear and tear on the joint surfaces. Not all cases of knee OA are related to a prior injury, however. Scientists believe genetics makes some people prone to developing degenerative arthritis. Obesity is linked to knee OA. Losing only 10 pounds can reduce the risk of future knee OA by 50 percent.
Scientists believe that problems in the subchondral bone may trigger changes in the articular cartilage. Normally, the articular cartilage protects the subchondral bone. But some medical conditions can make the subchondral bone too hard or too soft, changing how the cartilage normally cushions and absorbs shock in the joint.
Symptoms
What does knee OA feel like?
Knee OA develops slowly over several years. The symptoms are mainly pain, swelling, and stiffening of the knee. Pain is usually worse after activity, such as walking. Early in the course of the disease, you may notice that your knee does fairly well while walking, then after sitting for several minutes your knee becomes stiff and painful. As the condition progresses, pain can interfere with simple daily activities. In the late stages, the pain can be continuous and even affect sleep patterns.
Diagnosis
When you visit, Trainer's Choice, our physiotherapist will take a history and do a physical exam. The diagnosis of OA can usually be made on the basis of the initial history and examination.
Some patients may be referred to a doctor for further diagnosis. Once your diagnostic examination is complete, the physiotherapists at Trainer's Choice have treatment options that will help speed your recovery, so that you can more quickly return to your active lifestyle.
Our Treatment
Non-surgical Rehabilitation
OA can't be cured, but physiotherapies are available to ease symptoms and to slow down the degeneration. Recent information shows that mild cases of knee OA may be maintained and in some cases improved without surgery.
Medication
Patients may also want to consult with their doctor or pharmacist regarding the use of pain relief or over-the counter anti-inflammatory medication. Acetaminophen (Tylenol) is a mild pain reliever with few side effects. Some people may also get relief of pain with anti-inflammatory medication, such as ibuprofen and aspirin. Talk to your doctor or pharmacist if you have questions or concerns regarding these medications.
Medical studies have shown that glucosamine and chondroitin sulfate can also help people with knee OA. These supplements seem to have nearly the same benefits as anti-inflammatory medicine with fewer side affects. Many therapists feel the research supports these supplements and are encouraging their patients to use them.
Physiotherapy
Your physiotherapist plays a critical role in the nonoperative treatment of knee OA. Physiotherapy may be needed to ease pain and improve mobility, strength, and function. Our primary goals are to help you learn how to control symptoms, maximize the health of your knee and prolong the time before surgery is needed. Although the time required for recovery varies, you will probably progress to a home program within two to four weeks
We begin by recommending ways to calm pain and symptoms, which might include the use of rest, heat, or topical rubs.
Our physiotherapists then teach patients how to protect the arthritic knee joint. This starts with tips on choosing activities that minimize impact and twisting forces on the knee. People who modify their activities can actually slow down the effects of knee OA. For instance, people who normally jog might decide to walk, bike, or swim to reduce impact on their knee joint. Sports that require jumping and quick starts and stops may need to be altered or discontinued to protect the knee joint.
Our physiotherapist may suggest that shock-absorbing insoles placed in your shoes to reduce impact and protect the joint. In advanced cases of knee OA, or when the knee is especially painful, we may recommend a cane or walker to ease joint pressure when walking. People who walk regularly are encouraged to choose a soft walking surface, such as a cinder or grass track.
A new type of knee brace, called a knee unloading brace, can help when OA is affecting one side of the knee joint. For example, a bowlegged posture changes the way the knee joint lines up. The inside (medial) part of the knee joint gets pressed together. The cartilage suffers more damage, and greater pain and problems occur. The unloading brace pushes against the outer (lateral) surface of the knee, causing the medial side of the joint to open up. In this way, the brace shares the pressure and unloads the arthritic medial side of the joint. A knee unloading brace can help relieve pain and allow people to do more of their usual activities.
For mild cases of knee OA, our physiotherapist may give you a heel wedge to wear in your shoe. By tilting the heel, the wedge alters the way your knee lines up, which works like the unloading brace mentioned above to take pressure off the arthritic part of the knee.
We will use range-of-motion and stretching exercises to improve your knee motion. Our physiotherapist will also show you strengthening exercises for the hip and knee to help steady you knee and give additional joint protection from shock and stress. People with knee OA who have strong leg muscles have fewer symptoms and prolong the life of their knee joint. Your physiotherapist will also suggest tips for getting your tasks done with less strain on the joint.
Post-Surgical Rehabilitation
Physiotherapy treatments after surgery depend on the type of surgery performed. Rehabilitation is generally slower and more cautious after knee replacement procedures and certain types of tibial osteotomies. After simple procedures such as arthroscopy, you may begin fairly aggressive exercise therapy immediately.
Your physiotherapy treatments usually begin the next day after surgery. Our first few rehabilitation sessions are used to ease pain and swelling, help you begin gentle knee motion and thigh tightening exercises, and get you up and walking safely. You may need to use either a walker or crutches after surgery. We may instruct some patients to limit how much weight they place on the knee for about four to six weeks.
After going home from the hospital, a physiotherapist may see you for a short period of home therapy before beginning outpatient physiotherapy. Our outpatient treatments are designed to improve knee range of motion and strength and to safely progress your ability to walk and do daily activities.
At Trainer's Choice, our goal is to help you keep your pain under control, maximize knee mobility, and improve muscle strength and control. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
Trainer's Choice provides services for physiotherapy in North America.
Physician Review
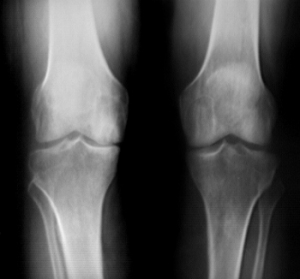
Radiological Testing
X-rays can help in the diagnosis and may be the only special test required in the majority of cases. X-rays can also help doctors rule out other problems, since knee pain from OA may be confused with other common causes of knee pain, such as a torn meniscus or kneecap problems. In some cases of early OA, X-rays may not show the expected changes.
Magnetic resonance imaging (MRI) may be ordered to look at the knee more closely. An MRI scan is a special radiological test that uses magnetic waves to create pictures that look like slices of the knee. The MRI scan shows the bones, ligaments, articular cartilage, and menisci. The MRI scan is painless and requires no needles or dye.
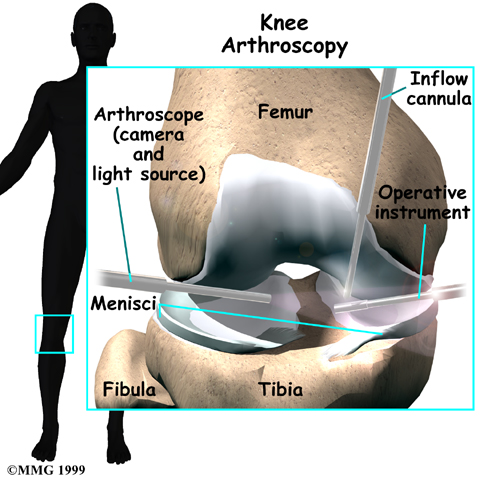
If the diagnosis is still unclear, arthroscopy may be necessary to actually look inside the knee and see if the joint surfaces are beginning to show wear and tear. Arthroscopy is a surgical procedure in which a small fiber-optic TV camera is inserted into the knee joint through a very small incision, about one-quarter of an inch long. The surgeon can move the camera around inside the joint while watching the pictures on a TV screen. The structures inside the joint can be poked and pulled with small surgical instruments to see if there is any damage.
Medication
Your physician may prescribe medicine to help control your pain. Acetaminophen (Tylenol) is a mild pain reliever with few side effects. Some people may also get relief of pain with anti-inflammatory medication, such as ibuprofen and aspirin. Newer anti-inflammatory medicines called COX-2 inhibitors show promising results and don't cause as much stomach upset and other intestinal problems.
Medical studies have shown that glucosamine and chondroitin sulfate can also help people with knee OA. These supplements seem to have nearly the same benefits as anti-inflammatory medicine with fewer side affects. Many doctors feel the research supports these supplements and are encouraging their patients to use them.
If you aren't able to get your symptoms under control, a cortisone injection may be prescribed. Cortisone is a powerful anti-inflammatory medication, but it has secondary effects that limit its usefulness in the treatment of OA. Multiple injections of cortisone may actually speed up the process of degeneration.
Repeated injections also increase the risk of developing a knee joint infection, called septic arthritis. Any time a joint is entered with a needle, there is the possibility of an infection. Most physicians use cortisone sparingly, and avoid multiple injections unless the joint is already in the end stages of degeneration, and the next step is an artificial knee replacement.
A new type of injectable medication has become available in the United States. Hyaluronic acid has been used in Europe and Canada for several years. Doctors inject three to five doses into the joint over a one-month period. The medicine helps lubricate the joint, ease pain, and improve people's ability to get back to some of the activities they enjoy. Some people have had good results for up to eight months after getting these treatments.
Surgery
In some cases, surgical treatment of OA may be appropriate.
 In cases of advanced OA where surgery is called for, patients may also see a physiotherapist before surgery to discuss exercises that will be used just after surgery and to begin practicing using crutches or a walker.
In cases of advanced OA where surgery is called for, patients may also see a physiotherapist before surgery to discuss exercises that will be used just after surgery and to begin practicing using crutches or a walker.
Arthroscopy
Surgeons can use an (mentioned earlier) to check the condition of the articular cartilage.
They can also clean the joint by removing loose fragments of cartilage. People have reported relief when doctors simply flush the joint with saline solution.
A burring tool may be used to roughen spots on the cartilage that are badly worn. This promotes growth of new cartilage called fibrocartilage, which is like scar tissue.
This procedure is often helpful for temporary relief of symptoms for up to two years.
Related Document: Trainer's Choice's Guide to Arthroscopy
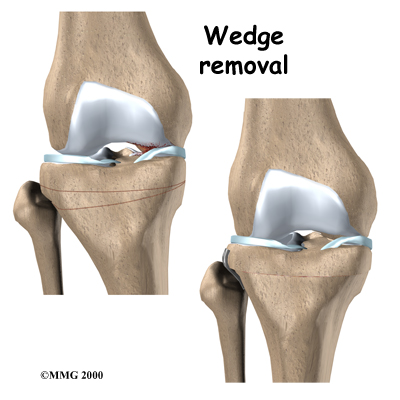
Proximal Tibial Osteotomy
OA usually affects the side of the knee closest to the other knee (called the medial compartment) more often than the outside part (the lateral compartment). OA in the medial compartment can lead to bowing of the knee. As mentioned earlier, a bowlegged posture places more pressure than normal on the medial compartment. The added pressure leads to more pain and faster degeneration where the cartilage is being squeezed together.
Surgery to realign the angles in the lower leg can help shift pressure to the other, healthier side of the knee. The goal is to reduce the pain and delay further degeneration of the medial compartment.
One procedure to realign the angles of the lower leg is called a proximal tibial osteotomy. In this procedure, the upper (proximal) part of the shinbone (tibia) is cut, and the angle of the joint is changed. This converts the extremity from being bowlegged to straight or slightly knock-kneed. By correcting the joint deformity, pressure is taken off the cartilage. A proper joint angle actually allows the cartilage to regrow, a process called regeneration.
This surgical procedure is not always successful. Generally, it will reduce your pain but not eliminate it altogether. The advantage to this approach is that very active people still have their own knee joint, and once the bone heals there are no restrictions on activities.
A proximal tibial osteotomy in the best of circumstances is probably only temporary. It is thought that this operation buys some time before a total knee replacement becomes necessary. The benefits of the operation usually last for five to seven years if successful.
Related Document: Trainer's Choice's Guide to Tibial Osteotomy
Artificial Knee Replacement
An artificial knee replacement is the ultimate solution for advanced knee OA.

Surgeons prefer not to put a new knee joint in patients younger than 60. This is because younger patients are generally more active and might put too much stress on the joint, causing it to loosen or even crack. A revision surgery to replace a damaged prosthesis is harder to do, has more possible complications, and is usually less successful than a first-time joint replacement surgery.
Related Document: Trainer's Choice's Guide to Artificial Joint Replacement of the Knee
Portions of this document copyright MMG, LLC.