Introduction
Physiotherapy in North America for Knee
Welcome to Trainer's Choice's patient resource about Hamstring Tendon Graft Reconstruction of the ACL.
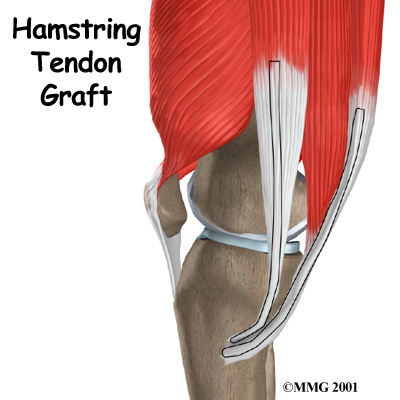
When the anterior cruciate ligament (ACL) in the knee is torn or injured, surgery may be needed to replace it. There are many different ways to do this operation. One is to take a piece of the hamstring tendon from behind the knee and use it in place of the torn ligament. When arranged into three or four strips, the hamstring graft has nearly the same strength as other available grafts used to reconstruct the ACL.
This guide will help you understand:
- what parts of the knee are treated during surgery
- how surgeons perform the operation
- what to expect before and after the procedure
Related Document: Trainer's Choice's Guide to Anterior Cruciate Ligament Injuries
Anatomy
What parts of the knee are involved?
Ligaments are tough bands of tissue that connect the ends of bones together. The is located in the center of the knee joint where it runs from the backside of the femur (thighbone) to the front of the tibia (shinbone).
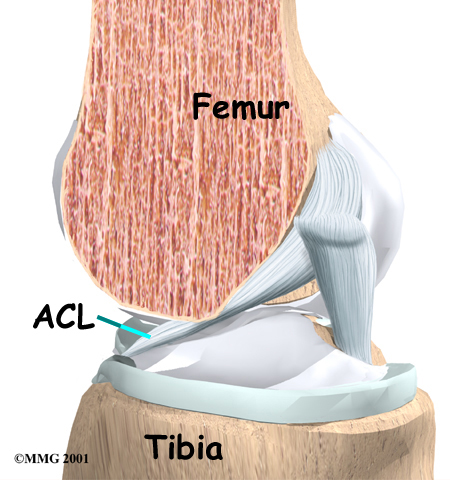
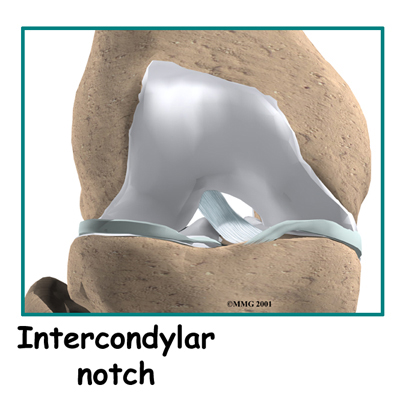
The ACL runs through a special notch in the femur called the and attaches to a special area of the tibia called the tibial spine.
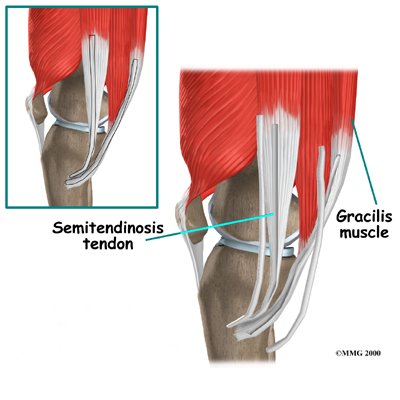
The make up the bulk of the muscles in back of the thigh. The hamstrings are formed by three muscles and their tendons: the semitendinosus, semimembranosus, and biceps femoris. The top of the hamstrings connects to the ischial tuberosity, the small bony projection on the bottom of the pelvis, just below the buttocks. (There is one ischial tuberosity on the left and one on the right.)
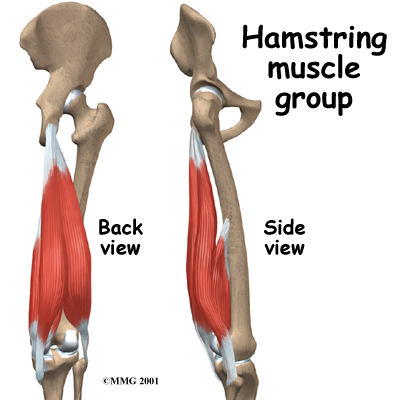
The hamstring muscles run down the back of the thigh. Their tendons and connect on each side of the tibia. The graft used in ACL reconstruction is taken from the hamstring tendon (semitendinosus) along the inside part of the thigh and knee. Surgeons also commonly include a tendon just next to the semitendinousus, called the gracilis.
The hamstrings function by pulling the leg backward and by propelling the body forward while walking or running. This movement is called hip extension. The hamstrings also bend the knees, a motion called knee flexion.
Related Document: Trainer's Choice's Guide to Knee Anatomy
Knee Anatomy Introduction
Rationale
What does the surgeon hope to accomplish?
 The main goal of ACL surgery is to keep the tibia from moving too far forward under the femur bone and to get the knee functioning normally again.
The main goal of ACL surgery is to keep the tibia from moving too far forward under the femur bone and to get the knee functioning normally again.
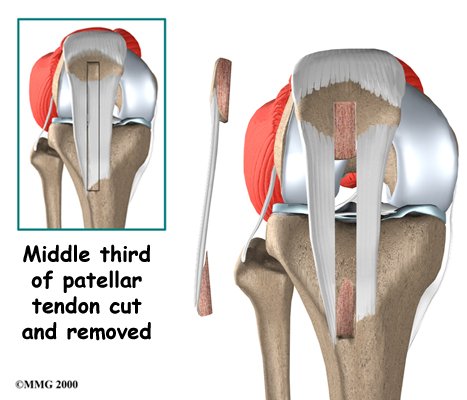
There are two grafts commonly used to repair a torn ACL. One is a strip of the patellar tendon below the kneecap. The other is the hamstring tendon graft. For a long time, the was the preferred choice because it is easy to get to, holds well in its new location, and heals fast. One big drawback to grafting the patellar tendon is pain at the front of the knee after surgery. This can be severe enough to prevent any pressure on the knee, such as kneeling.
For this reason, a growing number of surgeons are using grafted tissue from the hamstring tendon. There are no major differences in the final results of these two methods. When it comes to symptoms after surgery, joint strength and stability, and ability to use the knee, either method is good. However, with the hamstring tendon graft, there are generally no problems kneeling and no pain in the front of the knee.
Related Document: Trainer's Choice's Guide to Patellar Tendon Graft Reconstruction of the ACL
Preparation
What do I need to know before surgery?
You and your surgeon should make the decision to proceed with surgery together. You need to understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, you need to take several steps. Your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
You may also need to spend time with the physiotherapist who will be managing your rehabilitation after surgery. This allows you to get a head start on your recovery. One purpose of this preoperative visit is to record a baseline of information. Your therapist will check your current pain levels, your ability to do your activities, and the movement and strength of each knee.
A second purpose of the preoperative visit is to prepare you for surgery. Your therapist will teach you how to walk safely using crutches or a walker. And you'll begin learning some of the exercises you'll use during your recovery.
On the day of your surgery, you will probably be admitted to the surgery center early in the morning. You shouldn't eat or drink anything after midnight the night before.
Surgical Procedure
What happens during the operation?
Most surgeons perform this surgery using an arthroscope, a small fiber-optic TV camera that is used to see and operate inside the joint. Only small incisions are needed during for this procedure. The surgery doesn't require the surgeon to open the knee joint.
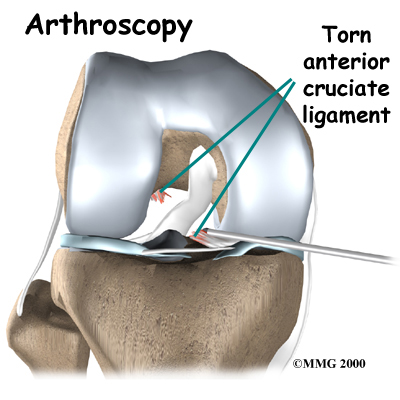
Before surgery you will be placed under either general anesthesia or a type of spinal anesthesia. The surgeon begins the operation by making two small openings into the knee, called portals. These portals are where the arthroscope and surgical tools are placed into the knee. Care is taken to protect the nearby nerves and blood vessels.
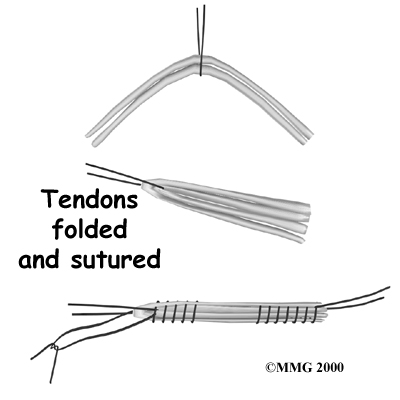
An incision is also made along the inside edge of the knee, just over where the hamstring tendons attach to the tibia. Working through this incision, the surgeon takes out the semitendinosus and gracilis tendons. Some surgeons prefer to use only the semitendinosus tendon and do not disrupt the gracilis tendon.
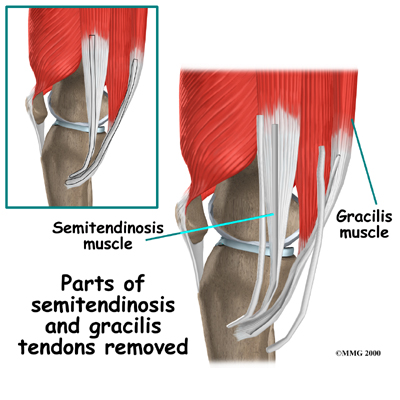
The tendons are arranged into three or four , which increases the strength of the graft. The surgeon stiches the strips together to hold them in place.
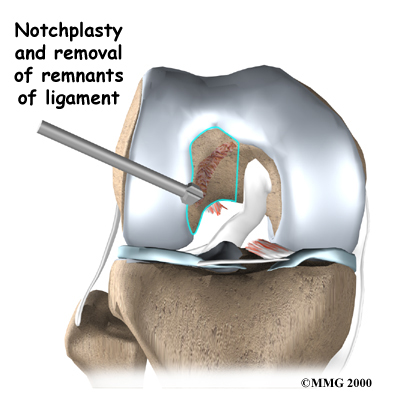
Next, the surgeon prepares the knee to place the graft. The remnants of the original ligament are removed. The intercondylar notch (mentioned earlier) is enlarged so that nothing will rub on the graft. This part of the surgery is referred to as a:
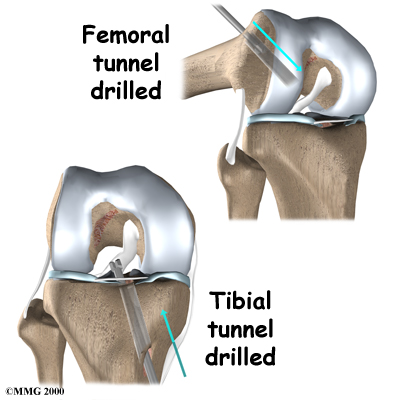
Once this is done, in the tibia and the femur to place the graft. These holes are placed so that the graft will run between the tibia and femur in the same direction as the original ACL.
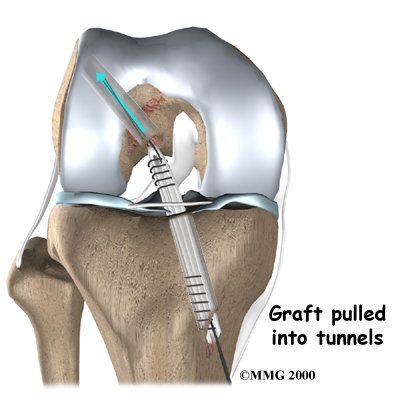
The graft is then through the drill holes. Screws or staples are used to hold the graft inside the drill holes.
To keep fluid from building up in your knee, the surgeon may place a tube in your knee joint. The portals and skin incisions are then stitched together, completing the surgery.
Complications
What can go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following hamstring tendon graft reconstruction of the ACL are:
- anesthesia complications
- thrombophlebitis
- infection
- problems with the graft
- problems at the donor site
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when blood clots form in the large veins of the leg. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible after surgery. Two other commonly used preventative measures include:
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Following surgery, it is possible that the surgical incision can become infected. This will require antibiotics and possibly another surgical procedure to drain the infection.
Problems with the Graft
After surgery, the body attempts to develop a network of blood vessels in the new graft. This process, called revascularization, takes about 12 weeks. The graft is weakest during this time, which means it has a greater chance of stretching or rupturing. A stretched or torn graft can occur if you push yourself too hard during this period of recovery. When revascularization is complete, strength in the graft gradually builds. A second surgery may be needed to replace the graft if it is stretched or torn.
Problems at the Donor Site
Problems can occur at the donor site (the area behind the leg where the hamstring graft was taken from the thigh). A potential drawback of taking out a piece of the hamstring tendon is a loss of hamstring muscle strength.
The main function of the hamstrings is to bend the knee (knee flexion). This motion may be slightly weaker in people who have had a hamstring tendon graft to reconstruct a torn ACL. Some studies, however, indicate that overall strength is not lost because the rest of the hamstring muscle takes over for the weakened area. Even the portion of muscle where the tendon was removed works harder to make up for the loss.
The hamstring muscles sometimes atrophy (shrink) near the spot where the tendon was removed. This may explain why some studies find weakness when the hamstring muscles are tested after this kind of ACL repair. However, the changes seem to mainly occur if both the semitendinosus and gracilis tendons were used. And the weakness is mostly noticed by athletes involved in sports that require deep knee bending. This may include participants in judo, wrestling, and gymnastics. These athletes may want to choose a different method of repair for ACL tears.
The body attempts to heal the donor site by forming scar tissue. This new tissue is not as strong as the original hamstring tendon. Because of this, there is a small chance of tearing the healing tendon, especially if the hamstrings are worked too hard in the early weeks of rehabilitation following surgery.
After Surgery
What should I expect after surgery?
You may use a continuous passive motion (CPM) machine immediately afterward to help the knee begin moving and to alleviate joint stiffness. The machine straps to the leg and continuously bends and straightens the joint. This continuous motion is thought to reduce stiffness, ease pain, and keep extra scar tissue from forming inside the joint. The CPM is often used with a form of cold treatment that circulates cold water through hoses and pads around your knee.
Most ACL surgeries are now done on an outpatient basis. Many patients go home the same day as the surgery. Some patients stay one to two nights in the hospital if necessary. The tube placed in your knee at the end of the surgery is usually removed after 24 hours.
Your surgeon may also have you wear a protective knee brace for a few weeks after surgery. You'll use crutches for two to four weeks in order to keep your knee safe, but you'll probably be allowed to put a comfortable amount of weight down while you're up and walking.
Our Rehabilitation
What will my recovery be like?
Patients usually take part in formal physiotherapy after ACL reconstruction. When you visit Trainer's Choice, our first few physiotherapy treatments are designed to help control the pain and swelling from the surgery. Our goal is to help you regain full knee extension as soon as possible.
Our physiotherapist will choose treatments to get the thigh muscles toned and active again. Patients are cautioned about overworking their hamstrings in the first six weeks after surgery. We may show you how to do isometric exercises for the hamstrings. Isometrics work the muscles but keep the joint in one position.
As the rehabilitation program evolves, our physiotherapist will choose more challenging exercises to safely advance the knee's strength and function. We'll use specialized balance exercises to help the muscles respond quickly and without thinking. This part of treatment is called neuromuscular training. If you need to stop suddenly, your muscles must react with just the right amount of speed, control, and direction. After ACL surgery, this ability doesn't come back completely without exercise.
Neuromuscular training includes exercises to improve balance, joint control, muscle strength and power, and agility. Agility makes it possible to change directions quickly, go faster or slower, and improve starting and stopping. These are important skills for walking, running, and jumping, and especially for sports performance.
When you get full knee movement, your knee isn't swelling, and your strength and muscle control are improving, you'll be able to gradually go back to your work and sport activities. Our physiotherapist may prescribe a functional brace for athletes who intend to return quickly to their sports.
Ideally, you'll be able to resume your previous lifestyle activities. However, athletes are usually advised to wait at least six months before returning to their sports. Most patients are encouraged to modify their activity choices.
You will probably be involved in a our progressive rehabilitation program for four to six months after surgery to ensure the best result from your ACL reconstruction. Although recovery time varies, in the first six weeks following surgery, expect to see the physiotherapist two to three times a week. If your surgery and Trainer's Choice rehabilitation go as planned, you may only need to do a home program and see your therapist every few weeks over the four to six month period.
Trainer's Choice provides services for physiotherapy in North America.
Portions of this document copyright MMG, LLC.

